Impingement syndrome

What is Impingement syndrome?
Put simply, it is the irritation of rotator cuff tendon under the acromion (a bony roof that covers the tendon).
There are a variety of causes ranging from abnormal shape of the acromion (curved or hooked) to dysfunction of the rotator cuff tendon that can lead to imbalance of the shoulder girdle and functional impingement as the cuff can no longer effectively compress the ball of the joint during overhead movements. This leads to dynamic impingement of the tendon. Sometime repetitive overuse as in athletes involved in throwing sports (javelin, fast bowling etc).
- Dull, sometimes nonspecific aching pain around shoulder
- Worse pain during overhead movements
- Difficulty in lying on the affected side, sleep may be disturbed.
It progresses slowly and usually without specific history of trauma. Diagnosis is confirmed by clinical examination using special tests. It is not uncommon to have an associated rotator cuff tear or other pathology like arthritis of the acromioclavicular joint (the ‘point’ of shoulder). An X ray and MRI or ultrasound scan aids the diagnosis.
Depending on the cause, like a rotator cuff strain, it can resolve with rest, NSAIDs and physiotherapy. However if there are structural problems like a curved acromion or calcified ligament, the condition may become chronic and surgery may be necessary.
- Initially this can be treated with Painkillers and anti-inflammatory medications. Physiotherapy can be useful to keep your shoulder strong and flexible but may be difficult in acute phase due to pain inhibition.
- Steroid injections are useful to reduce inflammation and control the pain, but effect is variable and usually temporary. It also works as a diagnostic aid when the diagnosis is in doubt. I usually do not do more than one injection as it can predispose the rotator cuff to rupture.
- If there is documented inflammation or partial tear of the rotator cuff tendon, PRP injection has more than 50% success rate.
- When conservative treatment has failed, surgery is necessary and gives predictable results. This involves removing the inflamed bursa (bursectomy) and shaving any spurs (acromioplasty).
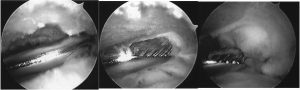
It is performed through keyhole (arthroscopy) and can be done as a day case (link to video).
- Pain management:
The shoulder will be sore and you will be discharged home with painkillers. Ice packs may also help reduce pain. Wrap frozen peas or crushed ice in a damp, cold cloth and place on the shoulder for up to 15 minutes. Please ensure you have covered the dressing / wound with some cling film before applying the ice pack to avoid getting the wound wet. - Wound management:
This is a keyhole operation usually done through two or three 5mm puncture wounds. There will be no stitches only small sticking plaster strips over the wounds. These should be kept dry until healed. This usually takes 7 – 10 days. - SLING:
Unless otherwise advised, this is for comfort only and should be discarded as soon as possible (usually within the first 2 to 4 days). Some people find it helpful to continue to wear the sling at night for a little longer if the shoulder feels tender. You are allowed full range of movements as your pain will allow.